INTRODUCTION
Scabies is an infectious skin disease caused by Sarcoptes scabiei var. hominis which is accompanied by intense itching [1]. Scabies infections can severely impair patients’ quality of life due to annoyance from itching and sleep disturbances. It also incurs significant financial losses for medical institutions due to ongoing infection control costs and negative publicity throughout a scabies outbreak [2,3]. In many countries, scabies has been neglected because it is not a notifiable infectious disease [4], which is the same in South Korea. It has been difficult to rapidly recognize the occurrence of scabies outbreaks. For this reason, the World Health Organization added scabies to the list of neglected tropical diseases in 2017 [5]. Scabies infections appear sporadically, making it difficult to determine the magnitude and seasonality of an outbreak in a population [4,6]. The prevalence of scabies at the national level varies greatly depending on the overcrowding of residential environments and the socioeconomic level including poverty rate [7]. In low-income countries in the tropical regions, prevalence is higher than 10%, while in developed countries, it is much lower [8,9]. Scabies is less prevalent in the temperate regions and more common in the tropical regions [9,10]. However, studies conducted in mid-latitude countries reported that scabies is more likely to occur in winter than in summer, resulting in an opposite dose-response relationship between temperature and scabies [4,11].
In developed countries, research on seasonality related to onset and reports on epidemiological characteristics such as the prevalence and tendencies of scabies in an entire population are lacking [4]. In this study, we assessed seasonal trends in relation to climate factors and estimated prevalence using scabies occurrence data in the national population.
MATERIALS AND METHODS
Extraction of scabies cases
South Korea has the National Health Insurance Service (NHIS) system that provides single-payer public health insurance for the entire population. It is run by a fee-for-service system and its payment is approved by the Health Insurance Review and Assessment (HIRA) service which reviews all claims. Using NHIS and HIRA data, research information can be obtained about disease diagnoses for the entire population [12]. In this study, data on subjects who were diagnosed with scabies (International Statistical Classification of Disease and Related Health Problems, Tenth Revision, code B86) were extracted from the main database of 2010 to 2017 and were used to estimate the prevalence by sex and age. Age was categorized into groups based on 10 year unit. The annual prevalence of scabies was calculated as the number of cases diagnosed per 1,000 by age group. The details of the use of medical institutions by patients diagnosed with scabies were divided into hospital and clinic. This study was approved by the Institutional Review Board of Sungkyunkwan University for its compliance with the Privacy Protection Act (SKKU 2018-01-008).
Meteorological factors
We developed a single model of total scabies cases in South Korea, meteorological factors were also included to represent the exposure level of the entire population. The national representative estimates of meteorological factors in South Korea were calculated based on data from 45 weather stations [13]. As the national average value, the Korea Meteorological Administration (KMA) has been using the average value of 45 weather stations that have been conducted stable and consecutive observations since 1973. In this study, monthly average temperature and monthly relative humidity in 2010–2017 were extracted from the above data.
Statistical analysis
Descriptive features of the prevalence stratified by demographic characteristics were presented. Non-linear regression analysis with a generalized additive model was used to determine the dose-response relationship between the monthly mean temperature and the number of monthly scabies cases. In this model, the number of monthly scabies cases was used as an independent variable, while the total annual population, average temperature, and relative humidity were used as dependent variables. To adjust for the decreasing trend of the overall number of scabies cases over time, we used the per capita gross national income (GNI) index, a socio-economic growth indicator at the national level. The per capita GNI data in South Korea were obtained from a Korean Statistical Information Service [14] as
where Casesij, Popy, and GNIy represent the number of scabies cases in i month of j year, the total population in j year, and per capita GNI in j year, respectively. AT(i-2)j and RH(i-2)j represent the national average temperature and relative humidity in i-2 month of j year, respectively.
The time difference between the number of scabies cases variable and the meteorological factors variable considers the delay between the initial infection and the final diagnosis. After a review of the existing literature related to the delay to diagnosis, the time of 2 months was applied in this study.
RESULTS
According to the HIRA service data, a total of 51,331 patients in 2010 and 42,436 patients in 2017 were diagnosed with scabies (Table 1). Until 2015, the number of cases was steadily decreasing, while the number of patients has rebounded slightly since 2016. The ratio of females to males diagnosed with scabies was 0.51:0.49 in 2010, but the gap between females and males continued to increase. In 2017, the ratio of females to males was 0.57:0.43, 1.33 times higher in females than in males. The number of scabies cases diagnosed in clinics has decreased by more than 10,000 (from 43,903 to 32,510) between 2010 and 2017. However, the number of scabies cases diagnosed at hospitals fluctuated without a certain tendency, but the proportion of cases diagnosed at hospitals among all cases steadily increased from 14% in 2010 to 23% in 2017. The proportion of cases by age group in the total number of scabies cases is consistently decreasing in the population of children, adolescents, and adults under 50 years of age. However, in the population over 50 years, the proportion of cases steadily increased over time. In 2017, in terms of the number of cases, the highest frequency occurred in the 50–59 years age group, followed by the 60- and 40-year age groups.
The prevalence of scabies per 1,000 persons was similar in children, adolescents, and adults under 50 years of age, ranging from 0.56 to 1.06, but the prevalence increased from age 50 to older age (Table 2). In particular, the prevalence of 2.88–3.86 per 1,000 persons in the group over 80 years old was 4–5 times higher than that of the younger age group. From 2010 to 2017, the overall prevalence decreased in all age groups, and the prevalence of scabies in the entire population decreased from 1.03 per 1,000 persons in 2010 to 0.83 per 1,000 persons in 2017.
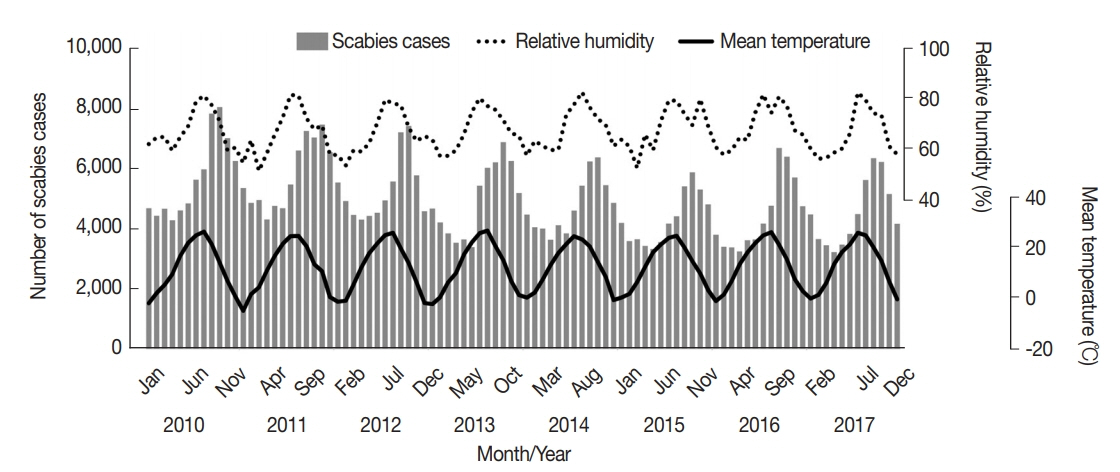
The occurrence of scabies in South Korea for the past 8 years showed a remarkable seasonality (Fig. 1). In October, approximately 6,800 people were diagnosed with scabies, the most cases were reported throughout the year. In April, approximately 3,700 people were diagnosed, the fewest cases were observed during the year. We examined the dose-response relationship between the monthly mean temperature and the monthly scabies cases when considering 2 months as the time delay effect from the initial infection to the diagnosis. Approximately 4,000 cases occurred at an average temperature of less than 5°C in the previous 2 months (Fig. 2). As the temperature increased, the number of scabies cases gradually increased. As a result, more than 6,000 cases occurred when the average temperature was 25°C or higher at 2 months prior.
DISCUSSION
This nationwide study demonstrated the decreasing annual trend of scabies in Korea. Its prevalence was highest in the elderly population while seasonality of scabies was closely associated with climate factors.
The pattern of the age-specific prevalence of scabies in low-income countries peaks during infancy and continues to decline until adulthood [8,10]. However, in developed countries in North America and Western Europe, the prevalence was evenly low in all age groups [10,11]. In the United Kingdom (UK), the average prevalence from 1997 to 2005 was approximately 2.5 per 1,000 persons and the overall female-to-male ratio was 1.24 [11]. The prevalence of scabies by age in South Korea has an opposite pattern to that in low-income countries. In South Korea, unlike other developed countries, the prevalence of scabies increases with age, presenting the highest prevalence in elderly people over 80 years of age. The female-to-male ratio for scabies cases in South Korea was 1.02 in 2010. However, since then, it has increased continuously and was 1.33 in 2017. From 2010 to 2017, the overall female-to-male ratio was 1.14, and more cases of women were reported, similar to that observed in the UK.
The high prevalence of scabies in the elderly can be considered from 2 aspects. One aspect is the increase in nursing homes for the elderly due to population aging and due to change toward the nuclear family [15]. The Korean government started providing long-term care insurance since 2008. As a result, the number of long-term care facilities is rapidly increasing. Also, the demand for nursing hospitals is increasing since the aging population and the number of elderly people living in a nursing home increased dramatically, from 7,864 in 2001 to 1,037,973 in 2012 [16]. In the early stage, this quantitative expansion caused problems with infection control and the quality of service was not managed properly. Since 2011, the quality level of all facilities has been evaluated and the results released to the public, thus qualitative control began to take place [17]. Long-term care facilities and hospitals have been still suspected as being the main route for scabies transmission [18–20], while patient transfers between hospitals and/or facilities have also contributed to transmitting scabies [18,21].
Our result supports the above estimations. For the last 8 years, the percentage of patients diagnosed with scabies in clinics has decreased by 9%, while those diagnosed in hospitals has increased by 9%. The other aspect is the high relative poverty rate in the elderly population, which is particularly high compared to developed countries in North America and Western Europe. However, the relative poverty rate in elderly Koreans is over 40%, which is extremely high compared to the relative poverty rate of 13.8% of the total population in Korea and the average relative poverty rate of 12.6% in the Organisation for Economic Co-operation and Development (OECD) member countries in 2015 [22–24]. Poverty in the elderly is accompanied by poor hygiene, overcrowding, and malnutrition, all of which are linked with a high prevalence of scabies [11,25].
The seasonality of scabies outbreaks has been reported in the data of a few specific age groups [4,11,26]. According to the survey on the young soldier population in Israel and on the children in the UK, more scabies cases were reported in winter than in summer. The seasonality of scabies in Europe seems to contradict our findings, however. The study in Israel reported the highest outbreak from December to February, with average temperatures around 10–15°C [4]. The report from the South Korean multicenter study showed that the highest outbreak was reported in October and November when average temperatures around 7–15°C, suggesting similar temperature ranges in both studies [18]. In our study, the number of scabies cases showed distinct seasonality from 2010 to 2017. The number of scabies cases began to increase in late summer and reached its peak in the autumn (September to November). From the winter, the number of scabies cases began to decrease again, and the lowest point was seen in the spring (March to May). This has been a very regular seasonal pattern, with a number of cases being 1.64 times higher in autumn than in spring (Fig. 1). When scabies peaked, the average temperature was similar to that of the previous studies at about 14.5°C.
Classically, the clinical presentation of scabies is typical as a pruritic skin eruption [27]. However, the clinical features may be atypically altered among institutionalized elderly patients, so pruritus may not be a predominant symptom [28]. For elderly patients residing in long-term care facilities with skin diseases as a result of poor hygiene, or as a result of communication difficulties due to cognitive impairment, the diagnosis can be delayed or errantly made as psoriasis or eczema [29]. Patients infected with scabies usually show clinical symptoms after an incubation period of 4–6 weeks [5,30]. The older the patient, the longer it takes to diagnose [18]. Because of these characteristics, it is known that scabies originating from elderly people living in long-term care facilities are the starting point of the spread [29,31–33]. Given the time delay from the initial infection to the diagnosis through the incubation period, most of the scabies cases diagnosed in autumn in South Korea were estimated to have started in summer. An analysis of the dose-response relationship between the average temperature and the number of scabies cases, the average temperature 2 months prior explained the increase in scabies cases.
This research has some limitations. First, access to raw data was only available for information on the number of diagnosed cases per month. Because previous studies suggested that it would take 4 to 6 weeks for scabies to be diagnosed, if data on the number of diagnosed cases per week could have been obtained, the dose-response curve in the number of diagnosed cases with changes in temperature could have been more elaborate. Second, the difference in temperature between regions in South Korea at the same time point is not large, but because the national representative average temperature and average relative humidity are used, the meteorological factors may not exactly match the spatial location of reported scabies. However, we presented the age-specific prevalence of scabies that is typically neglected disease by using insurance data for the entire population in South Korea. In addition, using meteorological data, we derived a dose-response relationship between the change in average temperature and the number of diagnosed scabies and provided the information on at what point in the year scabies cases could increase.
The main cause of the occurrence of scabies was previously considered due to a poor living environment. However, despite advances in medical technology and improvements in environmental facilities, recent outbreaks in developed countries increased in elderly care facilities due to diagnostic delay, medical staff indifference, and caregiver carelessness. Apart from socio-economic factors, when considering both the incubation period and the delayed diagnosis, the rising of average temperature in the summer season prior to about 2 months could account for the increasing of scabies in the autumn season. Population aging is rapidly progressing in South Korea, so the demand for long-term care facilities such as nursing homes is expected to increase steadily in the future. The understanding in the seasonality related to the average temperature in scabies and the identification of the prevalence according to the demographic characteristics will help to establish a strategy to control scabies.