Warning: mkdir(): Permission denied in /home/virtual/lib/view_data.php on line 81
Warning: fopen(upload/ip_log/ip_log_2024-04.txt): failed to open stream: No such file or directory in /home/virtual/lib/view_data.php on line 83
Warning: fwrite() expects parameter 1 to be resource, boolean given in /home/virtual/lib/view_data.php on line 84 Evaluation of enzyme-linked immunosorbent assay in serological diagnosis of human neurocysticercosis using paired samples of serum and cerebrospinal fluid
Evaluation of enzyme-linked immunosorbent assay in serological diagnosis of human neurocysticercosis using paired samples of serum and cerebrospinal fluid
Seung-Yull Cho,1Suk Il Kim,1Shin Yong Kang,1Duck Young Choi,2Jong Sik Suk,2Kil Soo Choi,3Young Soo Ha,4Chin Sang Chung,5 and Ho Jin Myung5
1Department of Parasitology, College of Medicine, Chung-Ang University, Seoul 151, Korea.
2Department of Neurosurgery, College of Medicine, Chung-Ang University, Seoul 140, Korea.
3Department of Neurosurgery, College of Medicine, Seoul National University, Seoul 110, Korea.
4Department of Neurosurgery, St. Mary's Hospital, Catholic Medical College, Seoul 150, Korea.
5Department of Neurology, College of Medicine, Seoul National University, Seoul 110, Korea.
Abstract
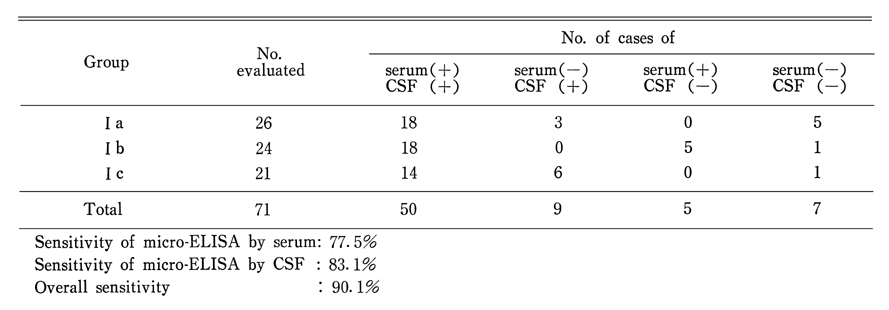
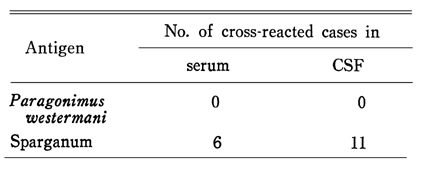
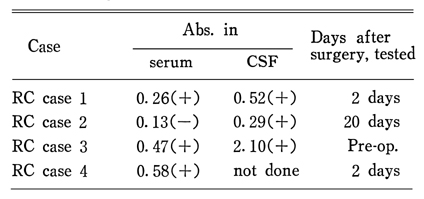
The applicability of micro-ELISA was evaluatd in human neuro-cysticercosis using paired samples of serum and CSF. A total of 355 cases who were mostly neurologic patients was subjected. Cystic fluid of C. cellulosae was used as antigen in protein concentration of 2.5 µg/ml. Serum was diluted to 1:100 and CSF was undiluted in the assay for the specific IgG antibody level. The differential criterion of the positive reaction was the abs. of 0.18 in both samples. The results were summarized as follows: The overall sensitivity of the micro-ELISA in 71 confirmed neurocysticercosis was 90.1%; the sensitivity by serum was 77.5% and that by CSF was 83.1%. CSF was a more sensitive and valuable material. Most of the false negative cases of neuro-cysticercosis showed far lower level of abs. rather than marginal. The overall specificity of the micro-ELISA in 52 confirmed other neurologic diseases was 88.5% ; the specificities by serum and by CSF were 94.2% respectively. Cases of other neurologic diseases did not show false positive reactions in both samples. When serum was assayed, taeniasis(2/18), sparganosis(2/20), paragonimiasis(1/56), clonorchiasis(1/15) and fascioliasis(1/1) cases showed cross reactions. When CSF was assayed, 2 of 10 neuro-sparganosis showed cross reactions while none of 9 neuro-paragonimiasis showed it. Out of 71 confirmed neuro-cysticercosis cases, 6 and 11 showed cross reactions by serum and CSF to crude extract antigen of sparganum; but no case did show it to crude extract antigen of Paragonimus westermani. Ventricular CSF showed low or negative levels of IgG antibody than lumbar CSF unless the lesion was at the lateral ventricle itself. Out of 4 racemose cysticercosis cases, 3 showed positive reaction in serum while all of 3 examined CSF were positive. The above results indicated that the serological test for detecting the specific IgG antibody by micro-ELISA using paired samples of serum and CSF was very helpful for clinical differentiation of neuro-cysticercosis from neurologic diseases of other causes.
Figures
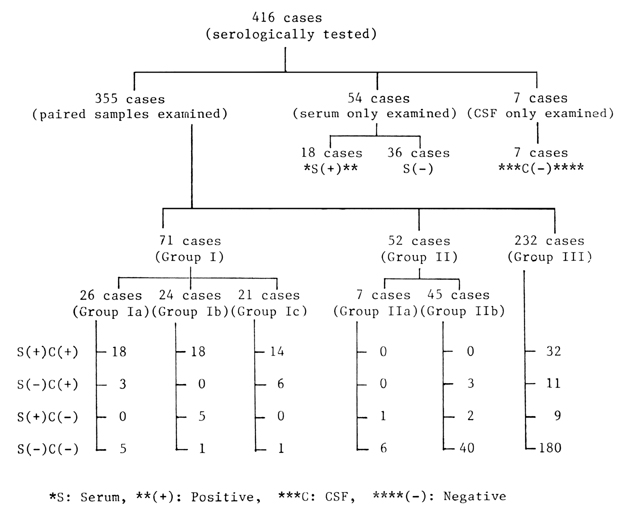
Fig. 1 General scheme of grouping in the present study.
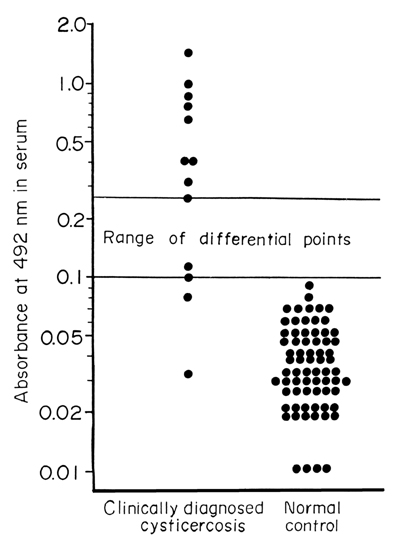
Fig. 2 Results of preliminary observation for Cysticercus-specific IgG antibody level in serum of 13 clinically diagnosed neurocysticercosis and 70 cases of normal controls.
Fig. 3 Ferquency distribution of 355 cases by the abs.(level of Cysticercus-specific IgG antibody) interval in serum and CSF.
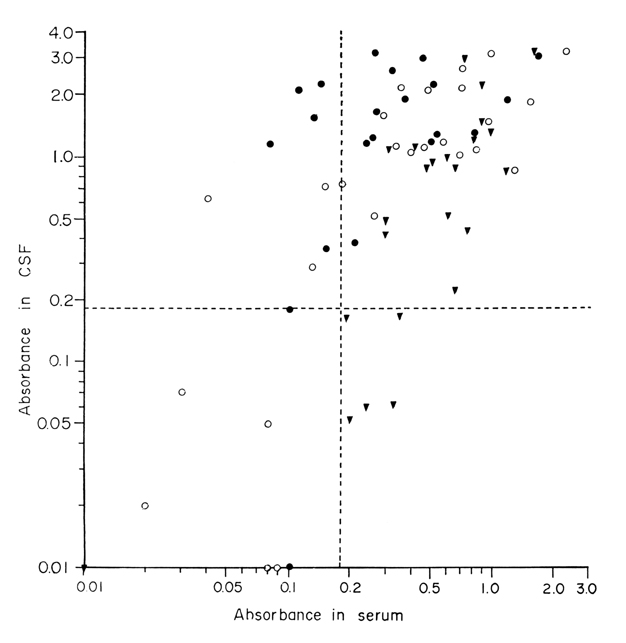
Fig. 4 Distribution of the abs. (specific IgG antibody level) in serum and CSF in confirmed neurocysticercosis patients (Group I). Open circle (○) : Neurosurgery confirmed (Group Ia), Closed triangle (▼) : Subcutaneous nodule biopsy and brain CT positive (Group Ib). Closed circle(●) :Multiple low densities in brain CT (Group Ic). Transverse and vertical dotted lines at the abs. of 0.18 are positive criteria.
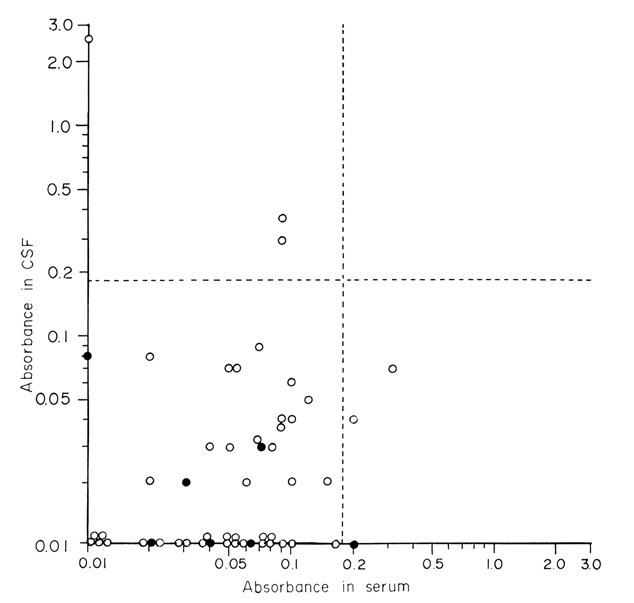
Fig. 5 Distribution of the abs. (specific IgG antibody level) in serum and CSF in confirmed other neurologic diseases (Group II). Closed circle (●) : Surgically Diagnosed other neurologic diseases (Group IIa), Open Circle(○) : Medically diagnosed other neurologic diseases(Group IIb). Dotted lines at abs. of 0.18 are the differential criteria of the positive reaction.
Fig. 6 Distribution of the abs. in serum and CSF in the remaining cases (Group III). Closed circle(●) : Clinically diagnosed as neurocysticercosis by follow-up CT after praziquantel treatment. Closed triangle(▼) : Biopsy confirmed muscular cysticercosis without neurologic symptoms or with normal brain CT. Open Circle(○) : Not confirmed cases of neuro-cysticercosis or other neurologic diseases. Dotted lines are differential criteria of the positive reaction.
Fig. 7 Relations of the abs. in serum and CSF in other parasitic infections to Cysticercus and homologous antigens. Transverse line at abs. of 0.25 is the positive criterion of other parasitic infections. Vertical line at abs. of 0.18 is criterion for cysticercosis. Dotted oblique line is y=x. Open circle(○) : Abs. in serum of paragonimiasis cases. Open triangle (▵) : Abs. is CSF of paragonimiasis cases. Closed circle (●) : Abs. in serum of sparganosis cases. Closed chiasis cases. Inverted open triangle (▿) : Abs. in serum of taeniasis cases. Double circle (◎) : Abs. in a serum of fascioliasis.
Tables
Table 1 The sensitivity of micro-ELISA in neuro-cysticercosis
Table 2 The specificity of micro-ELISA in neuro-cysticercosis
Table 3 Incidence of cross reactions in sera and CSF of other parasitic infections to Cysticercus antigen
Table 4 Incidence of cross-reaction in 71 cases of neuro-cysticercosis(Group I) to Paragonimus and sparganum antigens
Table 5 Results of serological tests in 4 racemose cysticercosis form the specific IgG antibody by micro-ELISA
References
1.
Arambulo PV, et al. Acta tropica 1978;15:63–67.
2.
Biagi F, et al. Rev Biol Trop 1961;9:141–151.
3.
Botero D, et al. Am J Trop Med Hyg 1982;31(4):810–821.
4.
Brink G, et al. Bol Chil Parasitol 1980;35:66–71.
5.
Carbajal JR, Palacios E, Azar-Kia B, Churchill R. Radiology of cysticercosis of the central nervous system including computed tomography. Radiology 1977;125(1):127–131.
6.
Cho SY, Hong ST, Rho YH, Choi SY, Han YC. Application of micro-ELISA in serodiagnosis of Human paragonimiasis. Korean J Parasitol 1981;19(2):151–156.
7.
Choi BK, et al. Chung-Ang J Med 1986;11(2):135–146.
8.
Coker-Vann M, Brown P, Gajdusek DC. Serodiagnosis of human cysticercosis using a chromatofocused antigenic preparation of Taenia solium cysticerci in an enzyme-linked immunosorbent assay (ELISA). Trans R Soc Trop Med Hyg 1984;78(4):492–496.
9.
Costa JM, Ferreira AW, Makino MM, Camargo ME. Spinal fluid immunoenzymatic assay (ELISA) for neurocysticercosis. Rev Inst Med Trop Sao Paulo 1982;24(6):337–341.
10.
Diwan AR, Coker-Vann M, Brown P, Subianto DB, Yolken R, Desowitz R, Escobar A, Gibbs CJ Jr, Gajdusek DC. Enzyme-linked immunosorbent assay (ELISA) for the detection of antibody to cysticerci of Taenia solium. Am J Trop Med Hyg 1982;31(2):364–369.
11.
Research needs in taeniasis-cysticercosis. Bull World Health Organ 1976;53(1):67–73.
12.
Flisser A, Pérez-Montfort R, Larralde C. The immunology of human and animal cysticercosis: a review. Bull World Health Organ 1979;57(5):839–856.
13.
Grogl M, Estrada JJ, MacDonald G, Kuhn RE. Antigen-antibody analyses in neurocysticercosis. J Parasitol 1985;71(4):433–442.
14.
Hong SK, et al. J Korean Neurosurg Soc 1978;7(2):417–423.
15.
Kim H, Kim SI, Cho SY. Serological Diagnosis Of Human Sparganosis By Means Of Micro-ELISA. Korean J Parasitol 1984;22(2):222–228.
16.
Koh YC, et al. J Korean Neurosurg Soc 1980;9(1):7–18.
17.
Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin phenol reagent. J Biol Chem 1951;193(1):265–275.
18.
McCormick GF, Zee CS, Heiden J. Cysticercosis cerebri. Review of 127 cases. Arch Neurol 1982;39(9):534–539.
19.
McLaren M, Draper CC, Roberts JM, Minter-Goedbloed E, Ligthart GS, Teesdale CH, Amin MA, Omer AH, Bartlett A, Voller A. Studies on the enzyme linked immunosorbent assay (ELISA) test for Schistosoma mansoni infections. Ann Trop Med Parasitol 1978;72(3):243–253.
20.
Miller B, Goldberg MA, Heiner D, Myers A, Goldberg A. A new immunologic test for CNS cysticercosis. Neurology 984 May;34(5):695–697.
21.
Mohammad IN, Heiner DC, Miller BL, Goldberg MA, Kagan IG. Enzyme-linked immunosorbent assay for the diagnosis of cerebral cysticercosis. J Clin Microbiol 1984;20(4):775–779.
22.
NIETO D. Cysticercosis of the nervous system; diagnosis by means of the spinal fluid complement fixation test. Neurology 1956;6(10):725–738.
23.
Rhoads ML, Murrell KD, Dilling GW, Wong MM, Baker NF. A potential diagnostic reagent for bovine cysticercosis. J Parasitol 1985;71(6):779–787.
24.
Rim HJ, Lee JS, Joo KH, Kim SJ, Won CR, Park CY. Therapeutic Trial Of Praziquantal (Embay 8440; Biltricide(R)) On The Dermal And Cerebral Human Cysticercosis. Korean J Parasitol 1982;20(2):169–190.
25.
Rodriguez-Carbajal J, Salgado P, Gutierrez-Alvarado R, Escobar-Izquierdo A, Aruffo C, Palacios E. The acute encephalitic phase of neurocysticercosis: computed tomographic manifestations. AJNR Am J Neuroradiol 1983;4(1):51–55.
26.
Salazar A, Sotelo J, Martinez H, Escobedo F. Differential diagnosis between ventriculitis and fourth ventricle cyst in neurocysticercosis. J Neurosurg 1983;59(4):660–663.
27.
Sotelo J, Escobedo F, Rodriguez-Carbajal J, Torres B, Rubio-Donnadieu F. Therapy of parenchymal brain cysticercosis with praziquantel. N Engl J Med 1984;310(16):1001–1007.
28.
Sotelo J, Guerrero V, Rubio F. Neurocysticercosis: a new classification based on active and inactive forms. A study of 753 cases. Arch Intern Med 1985;145(3):442–445.
29.
Tellez-Giron E, et al. Boletín de la Oficina Sanitaria Panamericanaq 1982;96(6):8–13.
30.
Yakoleff-Greenhouse V, Flisser A, Sierra A, Larralde C. Analysis of antigenic variation in cysticerci of Taenia solium. J Parasitol 1982;68(1):39–47.
31.
Zee CS, Segall HD, Apuzzo ML, Ahmadi J, Dobkin WR. Intraventricular cysticercal cysts: further neuroradiologic observations and neurosurgical implications. AJNR Am J Neuroradiol 1984;5(6):727–730.