INTRODUCTION
Toxoplasma gondii is an obligate intracellular parasite which infects both humans and animals as a zoonotic pathogen widespread in nature [1,2]. However, the prevalence of the disease and sources of infection vary among geographic regions with different climates, eating habits, and hygiene status [3-6].
Toxoplasmic retinochoroiditis is the major cause of visual impairment in high T. gondii endemic regions of the United States and the European nations, where it accounts for 30-50% of the posterior uveitis [7]. In Korea, however, the detection of retinal diseases caused by T. gondii is limited [8,9], and the seroprevalence of T. gondii has been reported to be around 2-7% among the general population in the 1980s [10,11].
Ocular involvement can be a result of acquired infection, or more commonly, a recurrence of the congenital form of the disease [12]. More recent reports support the view that acquired infections might be a more important cause of ocular diseases than previously assumed [13-15]. Toxoplasmosis is a progressive and recurrent disease, with which vision-threatening complications, such as retinal detachment, chorioretinal anastomosis, and choroidal neovascularization, may occur any time in the clinical course of the disease. For this reason, patients should be followed periodically to reduce the occurrence of the late complications.
In this study, we report the clinical features, recurrence rate, complications, treatment, and visual results of 10 Korean patients as the first series study of Korean cases with acute symptomatic ocular toxoplasmosis.
CLINICAL FEATURES OF CASES
We retrospectively analyzed the medical records of 10 consecutive patients of 9 males and 1 female diagnosed as active ocular toxoplasmosis at the Uveitis Service of the Ophthalmology Departments of Uijeongbu St. Mary's Hospital and Seoul St. Mary's Hospital from 2006 to 2010 and with at least 6 months follow-up. The demographic and general characteristics of the patients are listed in Table 1. Six of the 10 patients lived at northern areas of Gyeonggi-do or Gangwon-do (province), well-preserved wildlife areas for wild boar and deers near the demilitarized zone (DMZ) facing North Korea. Actually, 5 of 10 patients (50%) had the definite eating history of wild boar meat or deer blood.
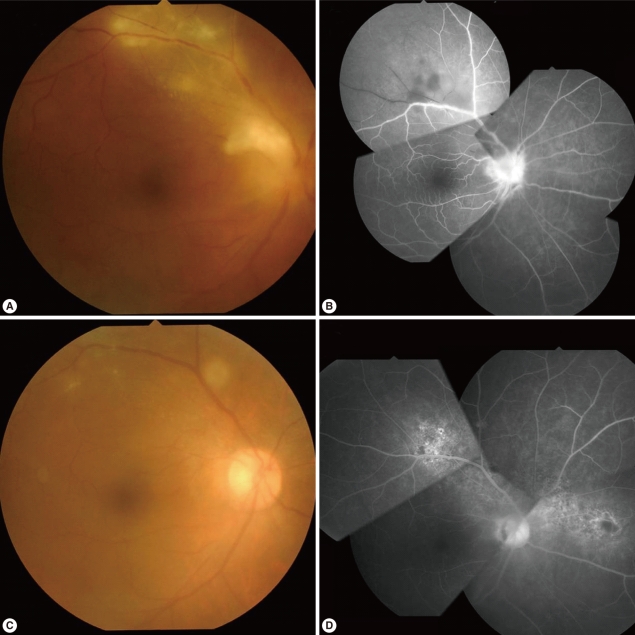
The diagnosis of active ocular toxoplasmosis was based on the acute onset of visual symptoms and the presence of characteristic focal retinochoroidal inflammation with or without a hyperpigmented retinochoroidal scar (Fig. 1) combined with serological evidence of Toxoplasma infection.
All of the patients underwent a complete ophthalmologic examination at each visit, including best-corrected Snellen visual acuity, slit-lamp biomicroscopy, tonometry, funduscopy with a Goldmann 3-mirror lens, and indirect ophthalmoscopy of fluorescein angiography. Initial visual acuity was better than 20/40 in 6 (60%) eyes, between 20/200 and 20/40 in 4 (40%) eyes, and less than 20/200 in none. At the initial examination, all patients had unilateral involvement without any scars except for 1 with pre-existing retinochoroidal scars. All active lesions were 2 disc diameters in size or smaller. Ocular findings included retinochoroiditis in 7 patients (70%), papillitis in 1 (10%), and periphlebitis in 4 (40%) eyes (Table 2). Active retinochoroidal lesion was located at the central retina in 2 patients (20%), peripheral retina in 3 (30%), and peripapillary retina in 2 (20%) eyes. All eyes with active lesions showed vitritis, and 7 eyes (70 %) had anterior uveitis. None of these patients had associated risk factors, such as immunosuppression, that might have caused atypical attack. Only 1 eye previously received systemic steroid treatment for posterior uveitis.
Serologic tests were performed by T. gondii-specific IgG antibody micro-ELISA [16], which detected all the sera as positive with OD from 0.26 to 0.78. Complete blood cell counts and erythrocyte sedimentation rate, liver and kidney function test, chest X-ray, and serum angiotensin converting enzyme level were within normal ranges in all patients. Serologic tests for syphilis and human immunodeficiency viral infection appeared as negative.
Our treatment protocol included clindamycin (300 mg, 4 times per day) and trimethoprim-sulfamethoxasol (160 mg and 800 mg each, twice a day). Oral corticosteroid therapy (prednisolone 30-40 mg, once a day) was initiated 1 week after the administration of antiparasitic treatment to check the drug response and always discontinued before antiparasitic treatment was stopped.
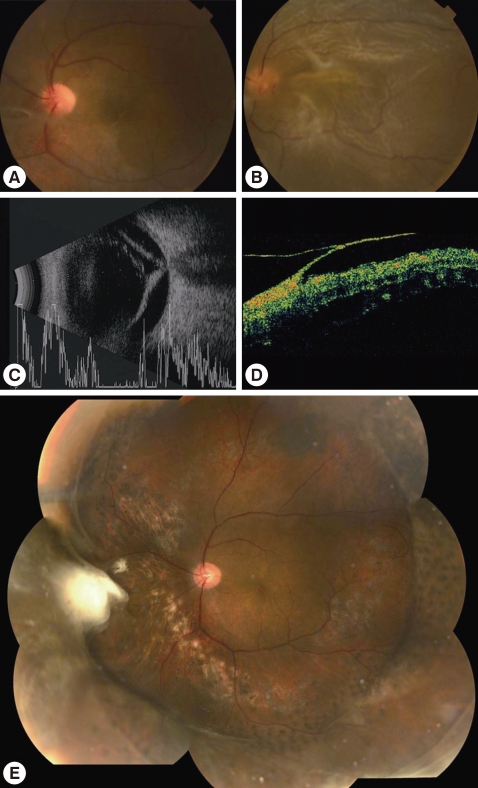
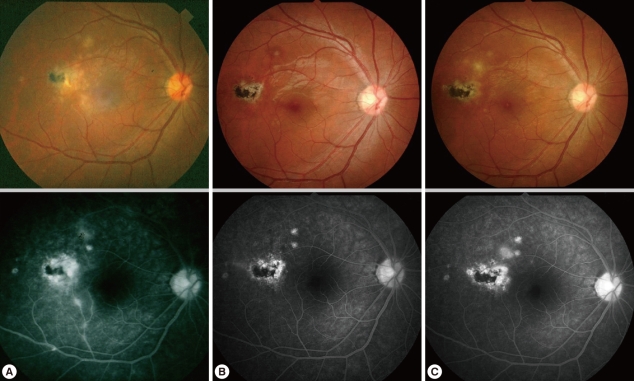
After the resolution of the presenting attack, visual acuity became equal or better than the initial in 9 patients (90%) and worse in 1 patient (10%). In the worsened patient, tractional retinal detachment near toxoplasmic scar was slowly progressed during the 2 years of following period, and then the patient underwent vitrectomy and scleral encircling. Anti-toxoplasmic IgG test was performed with vitreous sample in this patient, which resulted in a positive result (Fig. 2). Three (30%) patients had recurrence, of which 2 occurred within 6 months after the first attack and the other at 20 months (Fig. 3). Tractional detachment and a medication-associated complication (i.e., diarrhea) were reported during the follow-up period.
DISCUSSION
Ten cases of ocular toxoplasmosis were presented here with the typical clinical manifestations supported by positive serological antibody titers against T. gondii. Ocular toxoplasmosis is one of the most common types (30-50%) of infectious uveitis affecting the posterior pole in countries with high endemicity (30-80% among human population) of T. gondii infection [7]. In Korea, however, there is difference in toxoplasmic environments, such as low prevalence and titers of antibody caused by eating behaviors, pet-loving preferences, and residential changes [17]. Also, there is a significant difference in gender ratio; 9 of 10 patients were males. It may be due partly to the fact that still the social activities of males is more popular than females in Korea and also to a medicinal misbelief that raw viscera of wild animals had beneficial effects for man's stamina.
The fact that only 1 (10%) patient had pre-existing retinochoroidal scars in our study also supports the hypothesis that acquired infections are more frequent causes than congenital infections in ocular toxoplasmosis. Also, the recurrence rate (30%) was lower than that of other overseas studies [2,3,6], although the recurrence found in our study had limitations related with the short follow-up period and small number of cases as well. Though it may be due, in some degree, to differences in life style, such as eating habits and hygiene, it is necessary to find ethnic or genetic differences in standards of lives between Korea and other developed countries.
We chose a treatment strategy of administration of clindamycin and trimethoprim-sulfamethoxasol with oral corticosteroid therapy instead of more effective Fansidar (pyrimethamine-sulfadoxin, Roche). This was because of concerns about Stevens-Johnson syndrome (SJS) sometimes experienced during the treatment of toxoplasmosis, even though no reports relating to T. gondii infection and SJS have been reported so far in Korea.
Recurrence of ocular toxoplasmosis may be obvious when the pre-existing scars are observed. In our report, only 1 of 3 recurred patient showed pre-existing scars, which reflected that the others were newly infected or reactivated in the eye from a chronic infection with brain cysts [9]. A half of the patients resided in northern parts of Gyeonggi-do and Gangwon-do near the DMZ and had experience of consumption of wild boar meat or deer blood, which are assumed to have been from well-preserved nature in those regions. Furthermore, the number of stray cats, and accordingly the oocyst-shedding cats, has been increasing in those regions [18-20] as a risk factor for T. gondii infection.
Therefore, although rarely detected in clinical fields, T. gondii should be considered as an infectious pathogen responsible for the ocular symptoms, such as retinochoroiditis or uveitis. We recommend to check the antibody titers against T. gondii as a routine item for those patients.