INTRODUCTION
Myiasis is a pathological manifestation caused by fly larvae that are feeding on living or dead tissue in the host for a particular time and develops into parasites [1,2]. It is classified clinically by cutaneous and visceral types [3]. The cutaneous infection is the major clinical presentation and ulcerations are the main predisposing factor of myiasis, but it is a rare complication of advanced malignant tumors [1,4]. Human myiasis, a commonly neglected tropical disease, occurs worldwide, especially in tropical and subtropical countries with low socioeconomic conditions [4]. Myiasis has recently caused one of the most common travel-associated infestations, a crucial problem in non-endemic countries [5,6]. A total of 464 cases were reported from 79 countries in the literature survey for the period 1997–2017 [7], among which 150 cases (32.2% of the total cases) were reported from Asia (63 cases from South Asia, 57 cases from Western Asia, 21 cases from East Asia, and 9 cases from South-East Asia). However, there are few reports on myiasis in Myanmar. We report a rare case of myiasis in an old woman who suffered from ulcerative breast carcinoma.
CASE RECORD
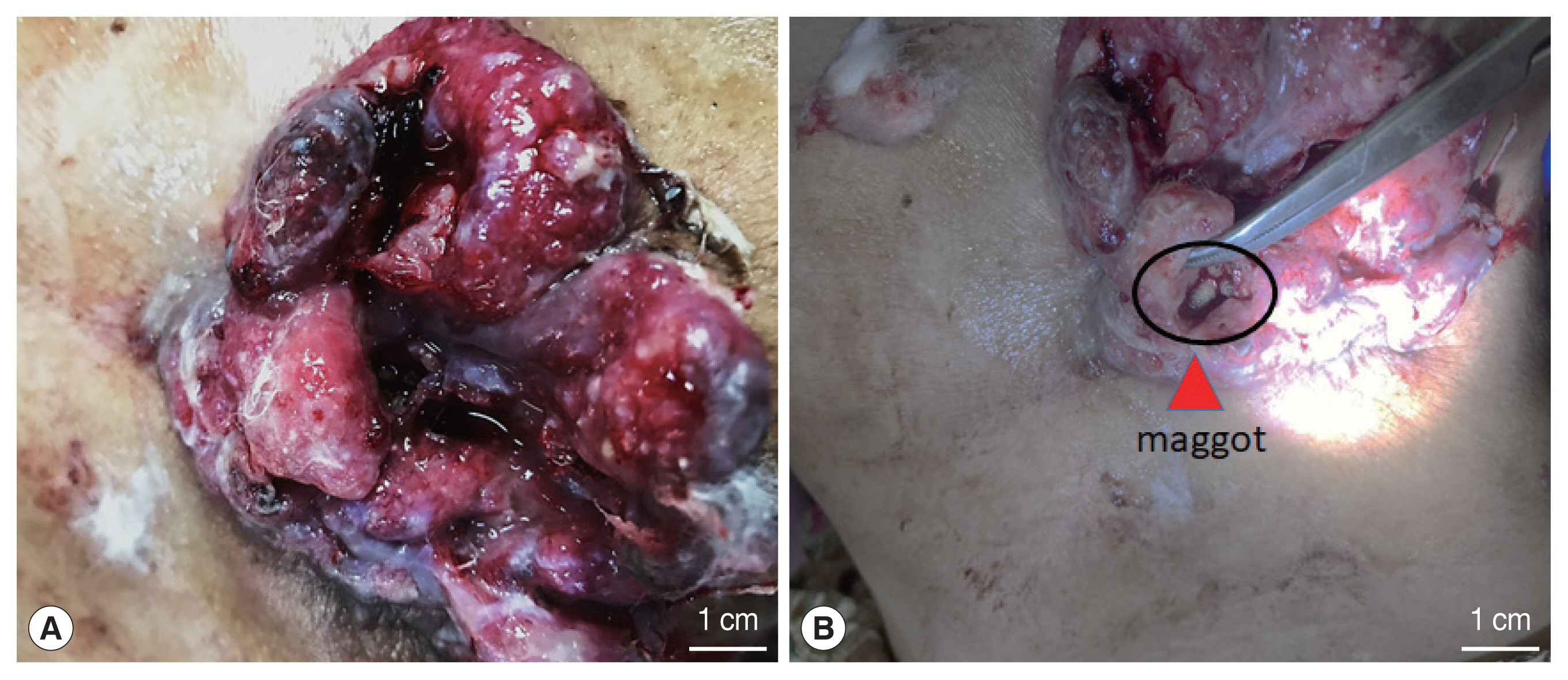
A 78-year-old female living in Dala Township, Yangon, Myanmar, visited our hospital with the chief complaints of irritation, itching, and pain in the ulcer lesion of the right breast for 3 weeks in 2019 (Fig. 1). She suffered from carcinoma in the lower inner quadrant of her right breast for 4 years. She was treated with traditional medicine, but an ulcer formed, and the lesion progressively worsened. The patient reported that blood and foul-smelling fluid oozed out from the ulcer and living creatures have been wriggling out of the ulcer lesion for 1 week.
On physical examination, approximately 6×7.5 cm sized ulcer was seen at the lower inner quadrant of the breast; the margin of the ulcer was ragged and swollen. Tissue invasions, local destruction, and necrotic areas were observed in areas where the patient experienced symptomatic pain, irritable sensation, and pruritus (Fig. 1). There were no palpable lymph nodes in both axillary regions and no abnormal mass or lesion of the left breast.
All maggots were manually removed with a clinical pincer under local anaesthesia (2% lignocaine) for easy removal and wound debridement. The ulcerous lesion was cleaned with Eusol daily and the patient was treated with Ampiclox (Amoxycillin 250 mg and Cloxacillin 250 mg) 500 mg 3 times a day for 2 weeks.
Larvae were preserved in 70% ethanol for further study. The identification of larvae was performed. The anterior and posterior air spiracles were removed from the bodies of maggots and examined under light microscope. The morphological characteristics of the peritreme of the posterior respiratory spiracles and the number of spiracular slit of larvae indicated a metallic fly (Fig. 2). Case record and photos of ulcer were taken and used with the permission of the patient and patient’s attendant No. 01/2019.
DISCUSSION
Wounds myiasis is found primarily in primary skin cancer. Other types of malignancies are also associated, but less common [3,8,9]. Wound discharge and necrosis are favorable conditions for blowflies to oviposit in these necrotic, hemorrhaging, or pus-filled lesions [10]. In addition, other predisposing factor such as a lack of hygiene and poor socioeconomic status, in the presence of an open wound, elderly age, chronic alcoholism, and chronic medical diseases are also involved [11, 12]. In our case, tissue invasion, pulsating lesion, and necrotic areas caused by larvae were observed in areas where the patient complained of symptomatic pain, movement sensation, and itching. Inflammatory changes of surrounding tissues and signs of secondary bacterial infection were observed all together (Fig. 1).
Although many species of flies have been associated with myiasis, larvae of family Calliphoridae and Sarcophagidae are the most commonly identified in malignant wound [13]. In the present case, microscopic examination of the peritreme of the posterior respiratory spiracles of larvae, the number of spiracular slit with actively free-motile nature indicated that these worms might be 3rd stage larvae of metallic fly (Fig. 2). This finding is in line with a previous report, in which reported that green bottle fly is the most common species identified for malignant wound maggot infestation [3].
Treatment of myiasis comprises removal of all visible larvae followed by debridement and consistent dressing changes daily [4,14]. Ivermectin has been suggested to be available. However, prevention and treatment of secondary bacterial infections and the inflammatory process, and removing the larvae should be the primary concern [4,14]. We used thorough and manual removal of maggots from the malignant wound and disinfection with Eusol solution as the best way to treat the patient. No medications for systemic treatment of myiasis was needed in this case. The patient was referred to the specialist hospital.
In conclusion, we report the first case of wound myiasis presenting as a complication of untreated or drug-induced ulceration caused by Myanmar traditional medicine. Environmental sanitation, personal hygiene, using tiny size mesh in windows, proper wound care, and using insecticides are possible factors to protect from flies for accidental myiasis.