Serodiagnosis of Echinococcosis by ELISA Using Cystic Fluid from Uzbekistan Sheep
Article information
Abstract
According to increase of travel, the cases of imported echinococcosis have been increasing in Korea. The present study was undertaken to develop a serodiagnostic system for echinococcosis in Korea. For diagnosis of echinococcosis, the fluid of Echinococcus granulosus hydatid cysts was collected from naturally infected sheep in Uzbekistan. Also serum samples of infected patients who were surgically confirmed were collected in a hospital in Tashkent, Uzbekistan. According to the absorbance of 59 echinococcosis positive and 39 negative control serum samples, the cut-off value was determined as 0.27. The sensitivity and specificity of ELISA with hydatid fluid antigen were 91.5% and 96%, respectively. The antigen cross-reacted with the serum of some cysticercosis or clonorchiasis patients. However, immunoblot analysis on the cystic fluid recognized antigenic proteins of 7-, 16-, and 24-kDa bands in their dominant protein quantity and strong blotting reactivity. In conclusion, the present ELISA system using hydatid cyst fluid antigen from Uzbekistan sheep is sensitive and specific for diagnosis of echinococcosis cases.
INTRODUCTION
Human echinococcosis is a zoonotic disease caused by cystic larvae of Echinococcus granulosus, E. multilocularis, E. vogeli, and E.oligarthrus [1,2]. Endemic areas include the Mediterranean regions, the Middle East, the Russian Federation, the People's Republic of China, eastern and northern Africa, Australia, South America, and some European countries. Humans are aberrant intermediate hosts, and the parasite does not grow to adults in human hosts [3,4]. Human echinococcosis is a tissue parasitic disease mainly of the liver or lungs but possibly in every organ of the human body.
The diagnosis of echinococcosis is mainly supported by both serology and images of radiography or ultrasound before surgery. Diagnosis of this disease before surgical intervention is important for proper and successful management. Various serological techniques were developed but ELISA is currently used for its serodiagnosis [5].
In Korea, a total of 34 cystic echinococcosis (CE) cases and 1 alveolar echinococcosis case have been reported in the literature based on identification of the parasite [6]. Most of the cases were imported, with the exception of 2 Korean cases in which the origin of infection was obscure [7]. A validated serodiagnostic test is necessary for proper management of CE-suspected patients in Korea. The present study aimed to develop a simple serodiagnostic system for human CE using E. granulosus cystic fluid antigen (EcAg) in Korea.
MATERIALS AND METHODS
Preparation of Echinococcus hydatid cystic fluid
Naturally infected sheep with hydatid cysts of E. granulosus were screened, and the cysts were collected in Uzbekistan [8]. The cystic fluid was collected and its supernatant was used as antigen after centrifugation for 30 min at 13,000 rpm at 4℃, and filtration using a syringe-driven 0.2-µm filter. Protein concentration of EcAg was measured using a Pierce BCA protein assay kit (Thermo, Rockford, Illinois, USA).
Human serum samples
A total of 158 serum samples were collected and used in this study. Among them, 59 were obtained from patients with echinococcosis who were confirmed by surgical observation from 2009 to 2010 in Uzbekistan. The mean age of the patients was 38.5±17.1 years (age range; 15-75 years). Men were 46 and women were 13 of the 59 patients. For the analysis of cross-reactions, 60 samples from patients with other parasite infections, which were retrieved from the serum bank of the Institute of Endemic Diseases, Seoul National University, Seoul, Korea, were applied to EcAg. As negative controls, 39 serum samples of healthy Korean individuals with no evidence of helminth infections were used. This study protocol was reviewed and approved by the institutional review board of Seoul National University College of Medicine (IRB No. C-0903-050-275). Informed consent was waived by the board.
Serology by ELISA
ELISA was developed to detect specific IgG antibodies in serum of echinococcosis patients with EcAg. For standardization of ELISA conditions with EcAg, chequerboard titrations of the antigen at concentrations of 0.5-50 µg of protein/ml and different dilutions of human serum and secondary antibodies were first performed. Based on the titration findings, the best concentration of protein for EcAg was defined as 100 µg/100 µl, and the best dilution of serum was determined as 1:100. The wells of polystyrene, flat-bottomed, 96-well plates (Costar-Corning, Cambridge, California, USA) were filled with 100 µl of coating buffer containing EcAg and incubated overnight at 4℃. Excess EcAg was removed by washing the wells 5 times with 250 µl of 150 mM phosphate buffered saline (pH 7.2) containing 0.05% (v/v) Tween 20 (PBST). The coated wells were blocked by adding 1% BSA in PBST at 37℃ for 1 hr and washed 5 times with PBST. The plates were incubated for 2 hr at 37℃ with sera diluted 1:100 in PBST (100 µl/well), 1 hr at 37℃ with anti-human IgG horse-radish peroxidase (Cappel, West Chester, Pennsylvania, USA) diluted 1: 24,000 with PBST (100 µl/well). After incubation in each step, the plates were washed 5 times with PBST. After adding 100 µl of tetramethyl benzidine (TMB; Pierce, Rockford, Illinois, USA) as substrate, the reaction was stopped with 4 N sulphuric acid (H2SO4), and the absorbance was measured at 450 nm. Based on ELISA reaction of echinococcosis patients and healthy control, the cut-off criteria absorbance was decided.
Sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE)
The EcAg (150 µl of antigen at a concentration of 1 µg/µl mixed with 150 µl of sample buffer composed of 50 mM Tris-HCl at pH 6.8, 2% SDS, 10% glycerol, 1% β-mercaptoethanol, 12.5 mM ethylenediamine tetraacetic acid and 0.02% bromophenol blue) was boiled for 5 min and then separated on a 10% SDS-PAGE at a constant current of 170 V for 1.5 hr. The individual antigen bands were then visualized by Brilliant blue R250 protein staining solution (Elpisbio, Daejeon, Korea).
Immunoblotting
The EcAg was separated by 10% SDS-PAGE and transferred onto polyvinylidene fluoride (PVDF) membrane. The membrane was cut into strips and blocked with 5% skim milk. The strips were incubated with serum samples (diluted 1:100 in 5% skim milk solution) at 4℃ overnight, and was followed by monoclonal anti-human IgG antiserum conjugated with horse-radish peroxidase (HRP; Dako, Glostrup, Denmark) which was used at a dilution of 1:2,000 with 5% skim milk. The reaction was visualized using ECL™ Western blotting detection reagents (Amersham, Piscataway, New Jersey, USA).
RESULTS
ELISA cut-off criteria
The cut-off value for EcAg ELISA was defined as over the mean absorbance plus 3 SD (0.063±0.054×3) of the values of 39 healthy controls (Table 1). The absorbances of 59 echinococcosis patients ranged from 0.112 to 0.974 (0.495±0.199). When the absorbance at 450 nm was blanked with the PBS, an absorbance of 0.270 was set as the optimum cut-off value to discriminate the positive and negative reactions (Fig. 1).

ELISA reactions of Echinococcus granulosus cystic fluid antigen for healthy control and helminthiases
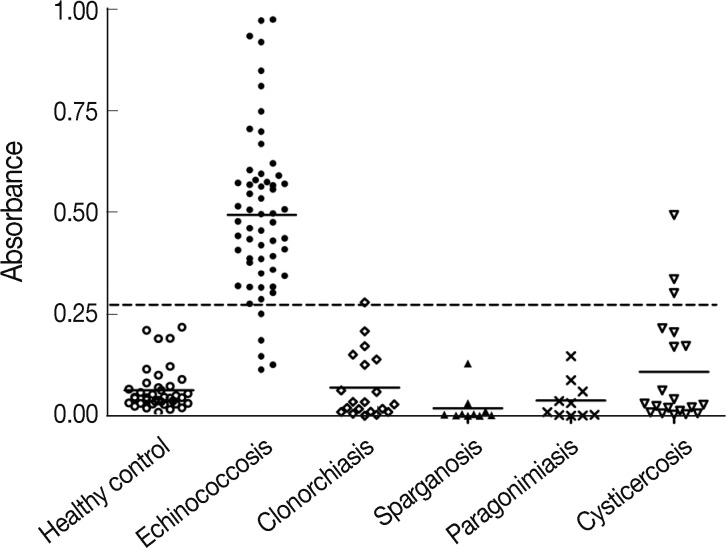
Distribution of ELISA absorbances to EcAg of cystic echinococcosis patients, healthy control and other helminthiases. Samples with an absorbance of less than 0.27 were defined as negative and those more than 0.27 as positive.
Determination of diagnostic values of EcAg ELISA
The mean absorbance of IgG ELISA using EcAg against serum specimens of negative control, echinococcosis and other helminthiasis patients are presented in Fig. 1. The ELISA for screening specific serum IgG antibodies for EcAg gave 91.5% (54/59) sensitivity and 96% (95/99) specificity (Table 2). The EcAg cross reacted with serum samples of cysticercosis and clonorchiasis.

Diagnostic value of Echinococcus granulosus cystic fluid antigen by ELISA
Immunoblot analysis of EcAg
Immunoblot analysis of EcAg showed many protein bands of 7-, 14-, 16-, 24-, 38-, 58-, 68-, 98-, and 116-kDa. Of them, 7-, 16-, and 24-kDa bands presented strong reactivity against human serum specimens from echinococcosis (Fig. 2). No serum samples from healthy control reacted with EcAg.
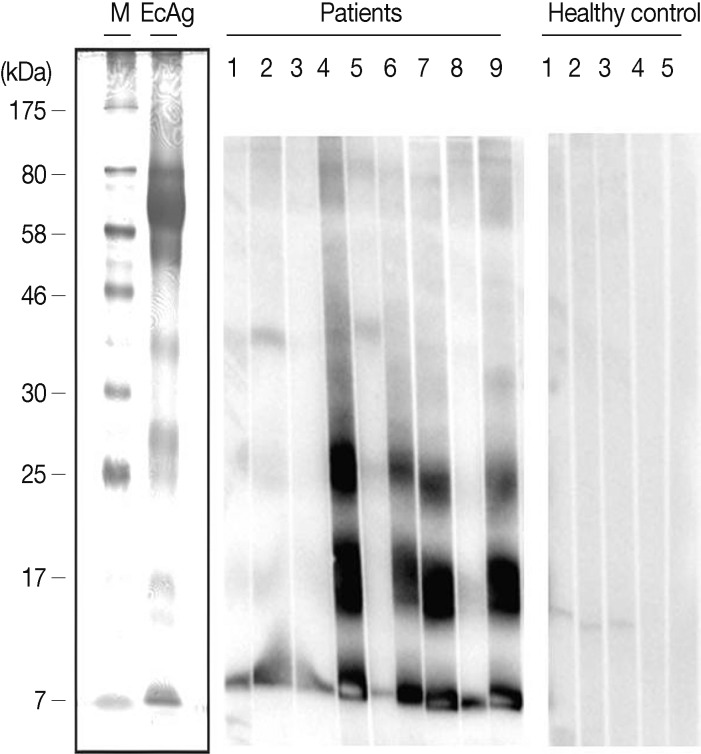
Immunobloting of EcAg probed with serum samples of infected patients (n=9) and healthy controls (n=5). M, size marker.
DISCUSSION
Our study developed a highly sensitive and specific ELISA system for screening of specific serum IgG antibodies to EcAg. The sensitivity and specificity of our ELISA were 91.5% and 96%, respectively. The positive and negative predictive values were 93.1% and 95%, respectively. Those diagnostic parameters were acceptable for a newly established serodiagnosis system.
It is known that the cystic fluid is a good antigen for serodiagnosis of human echinococcosis [5]. Although it is not scientifically new, establishing an ELISA system using EcAg for echinococcosis diagnosis in Korea is recordable. Since it is impossible to obtain the hydatid cyst from sheep in Korea, we collected the cyst in Uzbekistan where CE is endemic [9]. Our EcAg from Uzbekistan sheep showed good diagnostic values.
The cut-off value was set at absorbance of 0.27 of our system (Fig. 1). The absorbance was above the mean and 3 standard deviations of the healthy controls. None of them was positive by the cut-off absorbance. However, our ELISA system found 5 false negative cases of human CE. All of them were surgically confirmed but serologically negative. It is difficult to explain the reason of the false negative reaction. In other reports, a few false negative patients were recorded [10-13]. The serology negative finding suggests that some patients are immune-tolerant and produce specific antibodies weakly in their serum. Most of them were found in the active stage of CE [12,13]. It may be possible to detect the antigen in their serum when the patients are negative for antibody. The false negative reaction must be a topic of further research.
Cross-reaction in serology is common between helminthes of close taxonomical position. Human CE is caused mainly by E. granulosus, but 3 other Echinococcus species are able to cause human echinococcosis. The species of the genus Echinococcus and other Taeniid tapeworms must share their antigenic molecules which may induce the cross-reaction. We have screened serum samples of common tissue-invading helminthiasis in Korea including clonorchiasis, paragonimiasis, cysticercosis, and sparganosis. Of them, 3 (15%) of cysticercosis serum samples and one (5%) of clonorchiasis cross-reacted with our EcAg. The absorbances of the 3 cross-reacting cysticercosis serum samples were rather high above the cut-off value. The finding suggests that the false positivity of cysticercosis is consistently strong enough to confuse its serodiagnosis. It is necessary to differentiate serodiagnosis of cysticercosis and echinococcosis by other additional information in endemic areas of both helminthiases. One cross-reaction of clonorchiasis was noticed but the absorbance was on the borderline and the disease pattern is quite different. Therefore the false positive reaction with clonorchiasis is not practically significant. It is suggested to check cross reactions between echinococcosis and cysticercosis by multiantigen ELISA for its serodiagnosis.
Our EcAg included many protein bands from 7- to 80-kDa, but 7-, 16-, and 24-kDa bands were mainly antigenic to serum of patients by immunopblotting (Fig. 2). The immunoblotting pattern was same as that of previous studies [14-16]. The present EcAg which we used in this study was confirmed as the same strain of sheep E. granulosus by the immunoblotting pattern. Haghpanah et al. [15] analyzed diagnostic values of the 3 bands of purified antigen B from sheep EcAg and suggested their sensitivity 77%, 82%, and 82% for 8-/12-, 16-, and 20-/24-kDa bands, respectively. The sensitivity increased to 91% when either reaction of the 3 bands was considered together. Although sheep EcAg was the standard antigen for serodiagnosis of CE, the ELISA absorbance was compared by cross reactivity between cystic fluid antigens from human and animals [17]. The ELISA absorbance of CE patients was the highest with the antigen B, and with cystic fluid antigen from human, sheep, mice, and cows in a decreasing order. The finding suggested improved serodiagnosis by ELISA with the antigen B of sheep EcAg.
The present study had a few limitations. Our EcAg from Uzbekistan sheep should be screened for its cross-reactivity with alveolar echinococcosis serum. Further studies are warranted for this. Total numbers of negative or positive controls were not enough to make a concrete conclusion and more data are required. Especially any cross-reaction with other tapeworms should be evaluated more.
In conclusion, the EcAg of hydatid cysts from Uzbekistan sheep is a useful antigen for serodiagnosis of human CE. The ELISA system will help differentiation of CE from other cystic diseases in Korea.
ACKNOWLEDGMENTS
The present study was supported by a grant from the Center for Disease Control and Prevention, Ministry of Health and Welfare, Korea (800-2010023). The authors gratefully acknowledge Ms. Hye-Seong Kim for her technical assistance in ELISA.