Intestinal Helminthic Infections Diagnosed by Colonoscopy in a Regional Hospital during 2001-2008
Article information
Abstract
The present study investigated characteristics of 24 parasite infection cases detected during colonoscopy in a regional hospital from January 2001 to December 2008. Sixteen patients were confirmed with Trichuris trichiura infection, 6 patients were with Ascaris lumbricoides infection, 1 patient with Enterobius vermicularis infection, and 1 patient with Anisakis infection. Among them, 7 patients (43.8%) were asymptomatic. Colonoscopy findings were normal in 18 patients (75.0%). Among the patients with T. trichiura infection, colonoscopy showed several erosions in 2 patients (8.3%) and non-specific inflammation of the affected segment of the colon in 3 patients (12.5%). In 1 patient with anisakiasis, colonoscopy revealed a markedly swollen colonic wall. Stool examinations were performed before treatment in 7 patients (29.2%) and were all negative for parasite eggs or worms. These results suggest that colonoscopy is a useful diagnostic approach for parasitic infections even for asymptomatic patients and for patients with negative stool examinations.
Until the 1970s, intestinal parasitic infections, mostly soiltransmitted helminths, were prevalent in South Korea. Since the South Korean government tried to establish parasite control projects in the 1960s, the helminth egg positive rate has dramatically decreased from 84.3% in 1971 to 2.4% in 1997 [1]. The egg positive rate in 2004 was 3.7% and has appeared to have shown a small increase as compared to the survey conducted in 1997 [2].
Colonoscopy is a preferred examination strategy for colorectal cancer screening due to a greater sensitivity and specificity as compared to the use of other modalities [3]. Occasionally, colonoscopy can reveal unexpected findings, including the presence of parasite infections, even if patients are asymptomatic. There have been a number of case reports where colonoscopy identified the presence of adult worms by direct visualization [4-11]. The present study investigated the characteristics of parasitic infections detected during colonoscopy in a regional hospital during the past 8 years.
At Uijeongbu St. Mary's hospital, colonoscopies performed to identify cases of parasitic infections were reviewed during the period from January 2001 to December 2008. Our records contained 24 reports that identified parasitic infections discovered during colonoscopy. Corresponding patient records were evaluated to determine the age at the time of presentation, gender, presenting symptoms, reasons for the colonoscopy, and histopathological findings. All parasites identified after a colonoscopy were removed using biopsy forceps or polypectomy snares. For parasite examinations, specimens were sent to Department of Parasitology, The Catholic University of Korea (Seoul, Korea).
The number of total colonoscopy examinations performed within an 8-year period was 29,234. Twenty-four reports (0.08%) of parasitic infections after a colonoscopy were identified (Table 1). Parasitic infections included 16 Trichuris tricihura infections (66.7%), 6 Ascaris lumbricoides infections (25%), 1 Enterobius vermicularis infection (4.2%), and 1 Anisakis larval infection (4.2%). The mean age at the time of diagnosis was 46.5 ± 14.2 years (age range, 22-81 years). Twelve (50%) of 24 patients were men, with a male:female ratio of 1 : 1. Among 16 patients with T. trichiura infection, 4 patients (25%) were immigrants from South-east Asia. The anatomic location of T. trichiura was identified as the cecum for 8 patients (50%), the ascending colon for 6 patients (37.5%), at multiple sites in 1 patient (cecum and descending colon, 6.3%), and in the rectum for 1 patient (6.3%). Colonoscopy findings were normal in 18 patients (75%). Among patients with T. trichiura infection, colonoscopy showed several erosions in 2 patients (8.3%) and non-specific inflammations of the affected segment of the colon in 3 patients (12.5%). The anatomic location of A. lumbricoides was identified as the terminal ileum in 1 patient (16.7%), the cecum in 1 patient (16.7%), the ascending colon in 2 patients (33.3%), the descending colon in 1 patient (16.7%), and the rectum in 1 patient (16.7%). In A. lumbricoides infections, colonoscopic findings were normal except for a live Ascaris (Fig. 1). These roundworms were captured with polypectomy snares or biopsy forceps and retrieved alive. One patient with E. vermicularis had undergone colonoscopy for the evaluation of anemia. E. vermicularis was detected in the ascending colon. One patient with colonic anisakiasis was asymptomatic. The Anisakis worm was found and was extracted from the ascending colon. Colonoscopy demonstrated a markedly swollen colonic wall in 1 patient with colonic anisakiasis. Stool examinations were performed before treatment in 7 patients (29.2%), and all examinations were negative for both eggs and parasites. All patients were treated with anthelmintic agents after colonoscopic removal of parasites.

Intestinal parasitic infections found at colonoscopic examinations at Uijeongbu St. Mary’s Hospital during 2001-2008
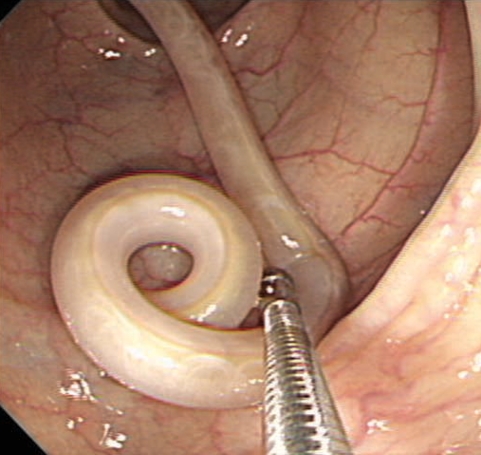
Endoscopic observation of Ascaris lumbricoides infection in a patient.
In the present study, all parasites identified by the use of colonoscopy were nematodes, including T. trichiura, E. vermicularis, A. lumbricoides, and Anisakis sp. Among the parasites, T. trichiura, also known as the whipworm because of the whip-like shape of the adult worms, was the most prevalent. The infection is mostly mild and asymptomatic. In our study, almost all T. trichiura in fections were asymptomatic or mild. However, when the parasite load increases, various symptoms, such as chronic lower abdominal pain, diarrhea, anorexia, and weight loss can arise. Moreover, colonic obstruction and perforation as well as lower gastrointestinal bleeding have been reported [12,13]. Among 16 patients with T. trichiura infection, 4 patients were immigrants from endemic areas, suggesting that sporadic cases occur occasionally due to immigration. In our study, the second most common parasitic infection determined was ascariasis. Most infections are asymptomatic. Only a minority of patients had clinical problems, mostly caused by a mobile adult worm mechanically blocking the lumen of the small intestine, main duodenal papilla, and appendix [14]. The A. lumbricodes infections seen in the present study were also asymptomatic or mild. Almost all previous case reports have shown that A. lumbricoides have been found in the appendix, cecum, ascending colon, or transverse colon [7,8]. However, our study demonstrated that A. lumbricoides could also be found in the descending colon or rectum. The pinworm, E. vermicularis has the broadest geographic distribution range and is the most common intestinal parasite encountered in the primary care setting [15]. It has been shown that a number of children with E. vermicularis infections could have endoscopic and histopathological features of nonspecific colitis [16]. However, we could not find abnormal colonoscopic findings in our patient. The stomach wall and the small intestinal wall are frequently involved sites for gastrointestinal anisakiasis. However, colonic anisakiasis is a rare condition. Although Anisakis infections can be asymptomatic, as in our case, infection may cause an acute onset of abdominal symptoms shortly after the ingestion of raw fish [11]. Colonoscopy frequently shows the presence of edematous mucosa, characterized by narrowing and multiple smooth and round protrusions. Furthermore, a variety of cases might be initially misdiagnosed as appendicitis, cancer, or inflammatory bowel disease, such as Crohn's disease or intestinal tuberculosis [17,18]. In this study, stool examinations failed to show the presence of any fecal eggs or parasites in 7 patients. Although stool testing is essential to determine the diagnosis of intestinal parasite infections, some difficulties can arise when infestation is caused by a limited number of male parasites [6]. Moreover, careful management, including sample collection, handling, and storage is necessary for optimal fecal assessment.
In conclusion, a careful colonoscopic examination should be performed for the identification and removal of parasites when symptomatic patients have a negative stool examination. Colonoscopy can be useful for the diagnosis of parasitic infections, even if patients are asymptomatic.